Deliberate Diagnosis Misdirection - Bias
Imagine if you opened a dictionary and the word "smart" didn't also point to "intelligent" or "doctor" did not also indicate "physician" might be a synonym. This is called cross-referencing. A good thesaurus or dictionary includes cross references.
The Diagnostic & Statistical Manual of Mental Disorders (5th edition) aka DSM-5 is no exception. No one is expected to memorize the DSM manual, although eventually therapists will be very familiar with the disorders they see most often of course. The book contains cross-references called "differential diagnosis" which creates a complicated but important web of disorders in a "see also" section that explains the difference between the diagnosis you're looking up and other diagnoses that might be mistaken for it so that the diagnostician can double-check themselves and make sure they're correct. This section is extremely important especially as some disorders include in their diagnostic criteria whether they take precedence over other disorders that might better explain a symptom set.
An example is (for example) Criteria E of ADHD says "The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g. mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal)." This criteria is supposed to indicate that this diagnosis is only used if something else more specific doesn't explain the symptoms. Something many doctors forget when diagnosing it. (Funny-not-funny note: it mentions dissociative disorders in Criteria E but not in Differential Diagnosis.)
So, normally most therapists won't immediately turn to Dissociative Identity Disorder when trying to puzzle out whether a client fits this or that diagnosis. They may be more familiar with the general criteria of another disorder and think maybe that's what's going on. So they start their search for what's going on for their client in the disorder(s) they are most familiar with, then do some cross-referencing work with other disorders to make sure they have the right diagnosis.
We created a chart to show which differential diagnosis points to which disorder or category of disorders (to make the chart neater, it's a mess already) � and only included the disorders that DID points to as they should likewise point back to DID as a rule. We omitted diagnoses that lead to needing medical diagnostics such as seizure disorders � that's outside the scope of the DSM to find out if they refer back and if they did it would likely come back into the DSM under conversion disorders. Also omitted are substance use disorder issues, as that's another level of complications. We consolidated BPD under personality disorders, since they don't point back to dissociative disorders anyway. And we also omitted "Unspecified Dissociative Disorder" as that's what is used at the ER when they don't know what's going on; it's mainly temporary and a one-way ticket with no differential diagnosis section.
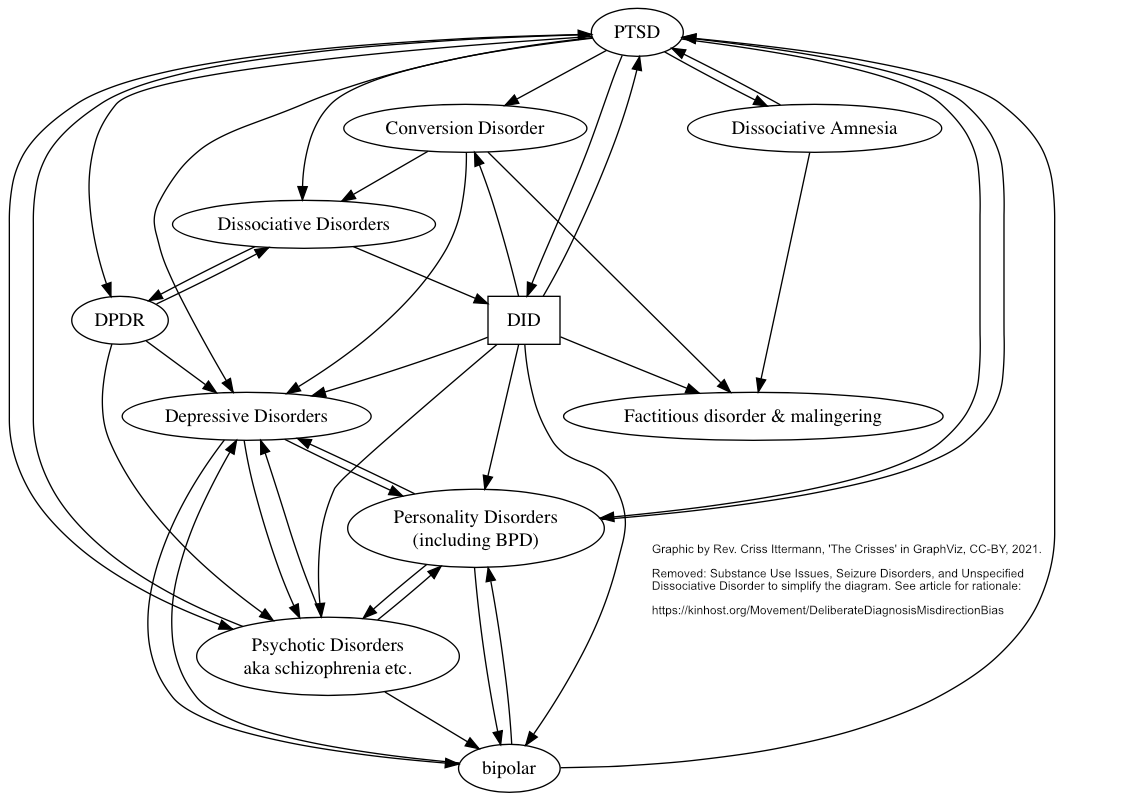
The chart ONLY covers the disorders that DID points to. Mapping the whole DSM would be well beyond our scope. It's possible there's an one-way reference from another disorder to DID that doesn't point back to that disorder, although unlikely.
Of the diagnoses that DID points to, the only diagnoses that point back to dissociative disorders are other dissociative disorders (DPDR, Dissociative Amnesia), conversion disorders (physical issues that cannot be medically explained, such as being blind one moment, and not the next � or non-epileptic seizures), and PTSD.
The only way, purely through the DSM, to get referred to DID is through PTSD or conversion disorder.
What does this look like? DSM-5 page 321, Conversion Disorder -> Differential Diagnosis -> Dissociative disorders. "Dissociative symptoms are common in individuals with conversion disorder. If both conversion disorder and a dissociative disorder are present, both diagnoses should be made."
When it says something like this, we just pointed it straight to "Dissociative disorders." So the therapist or clinician would have to dig through the whole dissociative disorders section and won't think of DID until they pass through the idea of "Is there a dissociative disoder?"
While no direct differential diagnosis assistance is done from PTSD to the individual dissociative disorders, it actually mentions each by name so we pointed to each of them, as there's at least a more direct reference. But it's still not really a full differential diagnosis explanation as it lacks any tips of what to look out for to figure out which of the headings to start with.
In other words, where other sections give a nice paragraph on how to tell whether say someone you suspect with bipolar may have a personality disorder instead, when it comes to DID a busy therapist is given a lot of homework to do if they don't just accept their first choice as the client's diagnosis and wing it from there.
The main thing to look at with this chart is how each disorder refers back to other disorders and vice-versa � unless it's a dissociative disorder. Only 2 non-dissociative disorders point back to dissociative disorders in general. Only 1 non-dissociative disorder points directly to DID (in a vague way).
The most common misdiagnoses for DID are schizophrenia (under psychotic disorders in the chart), bipolar and BPD (under personality disorders). Neither of these point back to DID. This is a deliberate omission from the DSM. Alan Francis, from the DSM-4 commission, basically confessed to wanting DID to be diagnosed less (than MPD was), i.e. to �make it less popular�. So every person who finally finds a DID support group and says they were in therapy for 20 years with the wrong diagnosis may want to send a love letter to Alan Francis.
For more about the deliberate nerf-ing of the DID diagnosis, and deliberately trying to obfuscate the diagnosis read Alan Francis's own words here: https://www.psychologytoday.com/us/blog/saving-normal/201401/multiple-personality-mental-disorder-myth-or-metaphor
Also of notable mention, the American Psychiatric Association is the body that publishes the DSM. They are likely more interested in keeping people in diagnoses with medications, as DID in itself doesn't have a psychopharmaceutical treatment. If they delay proper diagnosis and keep people diagnosed as schizophrenic or bipolar, they make more money (for the pharmaceutical industry via prescribing medications, via direct appointments with clients to tweak and monitor medications, and potentially kick-backs from pharmaceutical bonuses for prescribing specific patented medications). Just saying follow the money. *shrugs* The people treating DID are not the people writing the book. They are favoring diagnoses they profit from by these actions and inactions.
The next question is how many people have they harmed, how much, and whether or not there were any additional incentives to them doing this such as kick-backs from Big Pharma or insurance companies, etc.
If anyone decides to take legal action, feel free to let us know. We would not be a member of the class in a lawsuit about this topic as we told our therapist about the people in our head when we were 17 and have not been directly harmed by this issue (we have adamantly avoided psychiatric medication, too). It makes us really upset and angry after being in support groups for so long and hearing the heartbreaking stories of people who have been bouncing between therapists with the wrong diagnosis, or on the wrong medications, sometimes for decades. They should have gotten help and the correct support many many years ago. This needs to stop as soon as possible, as well. Some medications can cause permanent issues, so should only be used when medically necessary.
We heard rumors they're working on the DSM 5-TR and this is definitely an issue of extreme bias that the current DSM coalition needs to hear about.