Unification aka Final Fusion (FF), Full Final Merging, Integration, Alter Integration - an overview of the ISST-D Guidelines for treatment of adults with DID with much notes and suggestions
by the Crisses
Disclaimer
Some things below may be biased by our personal opinion of the process. It's important to note that we are not aiming for final fusion. We have not experienced it, nor attempted to fuse any of our headmates on purpose. We do achieve merges and blends that are synergistic and wonderful but temporary. None of us have spontaneously merged that we know of, although we have had fragments merge into headmates, both spontaneously and deliberately. We also have some very strong feelings about how therapists participate in the process, both in terms of pushing for it, or advocating for it, how they go about all the stages of the therapeutic process, etc. — mostly based on repeated feedback on experiences of DID systems at various stages in the processes below, and having read the ISST-D guidelines, and getting to see the mismatch between instructions on the one hand, and how they're actually carried out "in the field" on the other hand.
The Problem
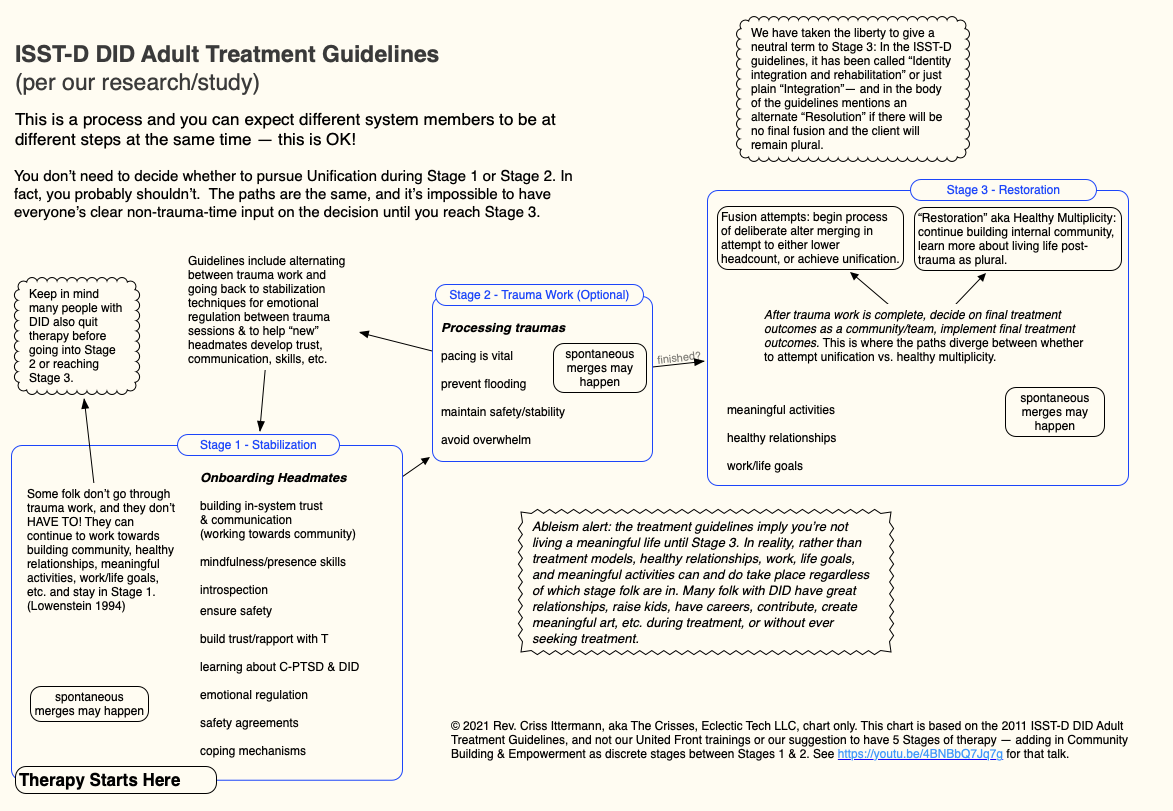
Stage 3 is where the real end goal for treatment needs to be set.
Unfortunately there's no one out there setting expectations for both client & therapist about this. The majority of folk out in the DID support community have made their decisions one way or another about this process before they're even done with Stage 1. There's years of work between Stage 1 and Stage 3; expectations & needs may change along the way.
The purpose of this article is to help educate both clients & professionals that no one needs to set the end goal of "unification" until they're in Stage 3 already. A therapist asking a handful of sessions into working with a client can send the client into a panic spiral, and clients walking in with a host asking for unification at the start of therapy is equally premature as they have probably not even achieved co-consciousness yet to get full consent of their system for long-term treatment goals.
When clients and professionals don't have realistic expectations they may end up suppressing system members and think the client has achieved unification. There are a lot of inept professionals out there who have no education on the suggested pathways for working with DID clients and are actively pluralmisic and singular-centric, and will push suppression tactics on their clients.
Background
Much of what's below is covered in depth in "Achieving 'Healthy' Multiplicity: The Case for 5 Steps" presented at the Plural Positivity World Conference in 2019, though the conference session is aimed towards therapists, and the article below may contain additional notes to the conference session � each is unique.
There is an article covering terminology issues, advocacy issues, & general debate over the process: Full Merging, Unification, Alter Integration ��Terminology, Controversy, & Issues.
Overview
This article is to give plural, DID and OSDD systems an overview of what this process ought to be. Unfortunately there are many unqualified therapists who shortcut this process, or who are using these ideas in a coercive manner, akin to conversion therapy.
So this process is outlined as what it should optimally be. To help empower your system so that y�all can selves-advocate.
This information, along with a special note for therapists, below, is also provided for therapists to check themselves and potentially realize when they are doing something that goes against the guidelines or is wrong or unethical.
There's no discernible difference in the process of recovery for DID systems up until phase 3 where the decision of whether to merge or to work on life skills as a team comes into play � so resources and treatment for DID systems up until that phase are identical. We have taken the liberty to provide links for further information or selves-help resources for many of the steps and processes mentioned below.
An overview of the ISSTD 2011 Adult Treatment Guidelines for DID
Downloadable PDF version: Attach:3Stages-ISSTD-2011.pdf
2011 Treatment Guidelines Overview in Full Text Only Version for Screen Readers New
Final Fusion Overview
Final fusion is a LONG process. It doesn't sneak up on you, it doesn't happen without work.
If a therapist is rushing someone to what they SAY is fusion, they're lying or horrifically mistaken, and potentially causing irreparable harm to the system, and it should never be therapist-led, only client-led.
There are important milestones before trauma work or final fusion should even be on the table:
Stabilization Phase
This phase includes client education, building rapport, developing coping mechanisms, and helping the client learn how to self-soothe, self-monitor, etc.
- System safety New, inside and out. This often includes making sure that internal folk have a safe space inside, that system kids are being taken care of, and other inner world work.
- System trust New, communication , internal community.
- finding New and comforting headmates New, onboarding New, recruiting system officers and crew (covered extensively in our book United Front: Recruits)
- finding and maintaining external supports such as case managers, support groups, friends, partners, clergy, coaches, peer support, etc. so that the DID system gets support between sessions. This can include having a System Safety Plan (we have an online course), hotline numbers, and a therapist not only offering crisis calls, but perhaps being explicit about what resources to use in various circumstances, and when it may be necessary to go to the ER. Many DID systems have experienced medical and other types of neglect, and honestly may not be aware of when to call on various parts of their support system and community resources.
- Client empowerment should be a mandatory part of the process from the start � and we believe that many therapists are negligent in missing this. Here's some articles, videos, conference sessions we've done that encourage client's to take back their own power:
- The Multiple Manifesto (brief video)
- Recruits, Rebels & Adventurers: How to get on the same page and pitch in to have a better life together
- Plural Activism & Selves-Advocacy
- Bootstrapping for �Healthy� Multiplicity
- Projection, Protection & Plural Power
- As Inside, So Outside & Vice Versa: Foundational Concepts in Building Internal Community
- Building a Reparenting-Focused Community
Having system "homework" and selves-help work New outside the therapy office can help move this phase along faster. Therapists can suggest the homework, or clients can take it on themselves � in any case anything that can be outsourced from therapy probably should. Y'all have enough work to do in therapy, that's why this process takes so long. Do work between sessions to make progress faster.
Trauma Work - what it is and how to do it New
Then trauma work�alternating with system stability and discovering lost and stuck traumaholders. This takes a long time, and done right isn't destabilizing because again it should all be client-led and the therapist constantly handing power back to the client system to direct the process and throttle the speed, and choose which traumas are ready to be worked on.
Along the way some spontaneous merges might happen. But only spontaneous, never coerced or finagled.
It's also possible that new headmates will surface during the process that weren't known before, or that now-time crises may require dropping back to the stabilization phase for a while and putting trauma work on hold. The DID system needs to be stable to dive into deliberate trauma work. There are inevitably traumas that come up during stabilization that need to be worked on immediately, versus seeking out traumas to work on while stable.
Whether to work on something at any given point needs to be client's choice otherwise it's likely to be retraumatizing.
See also Trauma Work New article for much more detail and thought on this process.
Merging
Then if the system has finished finding and working through trauma, discovering traumaholders, rescuing them, processing their stuff etc. to the point that all memories are recovered and all alters known, THEN if the client wishes to, a process of deliberate merging scan ensue. And that's another long process�until everyone is merged together. If this is truly what the client system desires, then we hope for their sake that it is a permanent solution for them.
The other option rarely mentioned by therapists is "Healthy Multiplicity" i.e. remaining plural, in recovery (per peer mental health definitions of "a process of ongoing self-care, monitoring, tweaking, learning, growing", not the medical-doctor definition of "ta-da you're completely cured you can now go neglect yourself again") and working out how to balance life as a team�but by this point, it's likely they have already been working on that for years, and can decide whether to continue therapy for check-ins and accountability, but can likely loosen up on the intensive therapy schedule and wean off of having intensive appointments.
Also of considerable importance during this stage are ensuring long-term strategies, coping mechanisms, support and skills for �reentry� whether as plural or singular to post-trauma-work life. How to deal with life without leaning heavily on dissociative coping mechanisms.
A common misconception is that being plural or switching is dissociative in nature. One can switch without needing to dissociate (therapists, you can disagree, but as someone living as plural, they are separate experiences which can overlap, but with high presence and high coconsciousness, they don't need to). But how to handle future adverse events without reaching for the preferred dissociative coping mechanisms is a new and important habit for anyone with a dissociative disorder, whether singular or plural.
It is still possible to dissociate without becoming plural again, and there are going to be times where folk dissociate just like normal people do. Being 100% present every minute of the day may be a goal, but it's not an achievable one (ask the Buddhist priest Nhat Hanh).
How Assured is Final Fusion?
Attempts at final fusion (FF) frequently fail. About 12% are successful (according to some short-term studies and those are not confirmed to continue to be successful in the long term � there are no longitudinal follow-up studies on this). This may be due to coercion, inexperience on the therapists' part, or many of our other notes here � but it also may be because this process strongly resembles conversion therapy. An attempt to force someone to be something they're not so that they "fit in" and "act normal" to please society � whether or not it's what they want for themselves, and often without their uncoerced consent.
Although this is not the author's desired outcome, it is sad because there are so many DID systems who long for final fusion, at least at the start of their journey. We hope that those who are successful are the ones who honestly wanted it, regardless of any pressure or coercion from their therapist or society. That would help us feel happy for them.
Do note that it's possible many DID systems would change their mind if they were given choices, and avoid the potential disappointment. They usually want final fusion while they aren't getting along and are fighting over who gets to live their life, and it's also a sign of a lot of internalized singular-centrism.
The fact is, most people who walk into the therapists' office plural (DID systems are plural, that's criteria A) � are going to remain plural the rest of their life. So rather than looking at being a DID system as a person who will eventually become singular � it's necessary to help them with teamwork and collaboration so they can be functional out in the world on their own. Symptoms will become manageable as a team, and they won't if they're fighting.
Then, as a team, they can decide whether or not final fusion, or any merging of headmates, is desirable for them as a group. Getting along better lubricates the merging process, even if respecting each other and getting along as a team may encourage them to give living their life as a group a chance. If it's working for them, it's no one else's business.
Over 70% Desire "Healthy Multiplicity" or "Functional Multiplicity"
In community surveys, which may misrepresent any specific client, over 70% of respondents wanted to remain plural after trauma work. As noted above, the needs or desires of those still in Stage 1 or 2 might change during treatment, but given the low success rate of final fusion, it's really on the professional community to reconsider their focus on unification as the preferred treatment goal, chosen by singular folk for plural folk.
Please see Functional or Healthy Multiplicity New for further discussion of these options.
A Special Note to Therapists
This information doesn't replace training, clinical supervision, CEUs, experience, etc. It's just a process outline and subject to change. This summary of the process is loosely based on the ISSD-D 2011 treatment guidelines, which are being revised at this time. But it also contains a couple notes regarding an epidemic of therapist abuse being reported in our community. Our observations, and suggested modifications to the 3-stage process, are clarified and expanded on in "Achieving 'Healthy' Multiplicity: The Case for 5 Steps" presented at the Plural Positivity World Conference in 2019.
So here's a quick note for therapists who are dealing with DID systems and attempting to lead them to final fusion:
- We have heard from too many systems where the "treatment plan" of final fusion was laid out at their FIRST SESSION with the therapist, or within 1-2 months of starting therapy, and it scared them away. It is a sign of an abusive therapist. You don't want to be that therapist. More about why:
- Don't talk about fusion until after trauma work is done. We can't say this loudly enough. It's not time to set goals for several years from now. You should not have this in any treatment plan with a new client. It's unrealistic. They have so many other steps to go through before it can even be on the table. It should not be your goal at this time or you may unconsciously rush through the steps needed and it should not be their goal at this time (see next bullet).
- You can ask what they want from therapy, they may mention fusion, but it may be best to remind them that this is a long process, and that it's not time to set goals that far out. If they think they are going to fuse within a few months, or even a year, and you allow them to have that idea you're doing them a grave disservice and it will encourage rushing through this process in ways they will likely hurt their system.
- It is not your life, you don't decide what is "best" for your client; they may very well decide they want final fusion, it is not your job to push them towards it. It must be the client's choice, no matter how convinced you are that this would be "best" for them. You don't live with the consequences, and you don't pay the bill. When it is finally time to discuss further treatment options, once trauma work is completed and it's time to discuss what's next, you need to give them options in the sense of more than one option for where to go from there. Traditionally there's 2 options. But there's a vast range between what is called Healthy Multiplicity "stay everyone we are now and how to stay healthy from here" and full fusion's "merge absolutely everyone in our system until we are a singular person". For example, some DID systems decide to merge many or even most of their headmates, and then live with healthy multiplicity with a lower system headcount from there. This is particularly helpful for systems with a very high headcount.
- Don't rush through Stabilization.
- Many therapists rush through the first phase. It's not glamorous to work on stabilization. They want to get to the "juicy details" and the parts that are highlighted in the famous books like this is some type of thriller movie. This process is not for your pleasure, or for you to save money on scary movie tickets. It is your job to do the least harm to your client. That means making sure you pay a lot of attention to the stabilization phase, and continually return back to it, to reinforce stabilization skills and ensure that the system is refreshed and relieved of pressures of trauma work between the potentially distressing trauma work sessions. Many therapists see DID clients more than once a week, so that the stabilization session comes shortly after a trauma work session. You may have to fight with insurance companies to cover this, but it is indicated while going through the trauma work phase.
- It's absolutely necessary along the way to help them build community and get along, preserve and recover system trust and safety inside, etc. because either they will decide to attempt fusion as a team and work together on it, or they won't ever be truly ready to do trauma work and will be destabilized constantly and it will be a really horrific process for them. Building community and trusting each other is also supportive of final fusion. It's much easier to see "becoming one" with someone you love and get along with than someone you hate and fight with. Keeping the system divided enforces amnesiac boundaries, increases anxiety and symptoms, and keeps the system hobbled with dysfunction throughout their whole life outside the therapy office. This is such an important step, that we suggested it as a separate autonomous phase of the process in our conference session.
- The client has to self-regulate during the trauma phase. The empowerment step that we suggest to add to the stabilization phase is extremely important (it's one of the steps we break out into an autonomous step in our conference session as a strong suggestion to the ISST-D to fix this oversight). They have to determine which traumas are ready to be worked on and when and how often, and how big, and when to stop. You are there to teach them to self-regulate. You cannot be their external self-regulation for them � that's disempowering, infantilizing, and dangerous. They need to learn to live without their therapist, and how to take care of themselves between sessions.
- Many therapists allow DID clients to lean on them, rather than lean on their system for support, or find external and supplemental support resources. While this may help the therapist feel needed, and powerful, and so on � it's not about that. The client DID system is not there to bolster your ego. You are not their savior, you're their consultant. We go into many reasons this is not a good idea in our article on Re-parenting.
- That said, this is another reason why we break out the building community phase into a separate step in our conference session. It can't be skipped over. Therapists who attempt to break up the system, suppress headmates, push them into a "king of the hill" formation where one fronts and everyone else stays in the back and never front or don't front in therapy are doing their system a grave disservice in terms of self-regulation, stabilization, protection, and recovery. It doesn't work that way. Employing singular-person methods on a plural system is not leveraging the strengths of being plural in the process of recovery and trauma work. It creates system distrust, increases anxiety, increases system sabotaging. You forcing your ideas of how they should behave and who should be allowed to engage in the therapeutic process on their system is a power & control move on someone who has repeatedly been disempowered and controlled by others. It perpetuates the abuse cycles that you're supposed to be helping them to recover from. Any demand to speak "only to the host" or some other headmate, to only allow certain alters to front, or to tell certain alters they're not allowed to front is the therapist overstepping the plural system's boundaries and continuing the cycle of violence against them.
- Take good care of yourself.
- Please revisit countertransferrance issues from your training, it's a known issue with DID clients. DID therapy is best with more than the usual disclosures from a therapist: trust & rapport is hard to build and maintain with folk with C-PTSD. We've been betrayed a lot. We will seek out connection, and you need to manage what is enough to build rapport vs too much and the client will attempt to attach in unhealthy ways and parentify the relationship.
- Also, we can't emphasize that you take care of yourself enough. This is hard work. Intense. You need the stabilization sessions as much as your client does. Do not be an adrenaline junkie and push this on your clients to stay in the heightened "exciting" work of trauma work all the time. You're going to hear things that no one else has heard these people say before. It's going to hurt to hear it. Stay human, stay humane. Don't push them, and don't push yourself. You want to make sure neither of you are getting avoidant, but you also need frequent breaks.
- That said, you do need to be absolutely certain where your own boundaries are and defend them gently, kindly, but firmly. You may have to tell some of your plural client system members that they are not allow to do or say some things to you, that that's not acceptable in the professional relationship. You may need to remind them that they hired you, and that you are there as a consultant to help them move through this process. You may need to put the ball back in their court, but also keep them from taking that ball and trying to play dodgeball with it without your permission.
<< DBT New | ManualTOC | Hypnotherapy New >>
See Also
- 2011 ISSTD Treatment Guidelines Graphic Text Only New
- Community Division: Endogenic vs. Traumagenic New
- Full Merging, Unification, Alter Integration ��Terminology, Controversy, & Issues
- Functional or Healthy Multiplicity New
- Hypnotherapy New
- Please make yourself at home - Part 2
- Stuck Residents aka stowaways, lost souls, non-coaware identities, emotional parts, etc. New
- To the Psych Community
- Trauma Work - what it is and how to do it New
- Treatment Modality Index New
- Who Am I Right Now?